Intense Module 1
Introduction

EXPLANATORY NOTES
INTRODUCTION
Spirometry (meaning the measuring of breath) is the most common of the pulmonary function tests (PFTs). It measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled. Spirometry is helpful in assessing breathing patterns that identify conditions such as asthma, pulmonary fibrosis, cystic fibrosis, and COPD. It is also helpful as part of a system of health surveillance, in which breathing patterns are measured over time.
Spirometry generates pneumotachographs, which are charts that plot the volume and flow of air coming in and out of the lungs from one inhalation and one exhalation.
Some of the basic terminology used for spirometry:
- TLC (Total lung capacity) :The volume in the lungs at maximal inflation, the sum of VC and RV.
- TV(Tidal volume): That volume of air moved into or out of the lungs during quiet breathing (TV indicates a subdivision of the lung; when tidal volume is precisely measured, as in gas exchange calculation, the symbol TV or VT is used.)
- RV(Residual volume): The volume of air remaining in the lungs after a maximal exhalation
- ERV (Expiratory reserve volume): the maximal volume of air that can be exhaled from the end-expiratory position.
- IRV (Inspiratory reserve volume) :the maximal volume that can be inhaled from the end-inspiratory level.
- IC(Inspiratory capacity): the sum of IRV and TV.
- IVC (Inspiratory vital capacity): the maximum volume of air inhaled from the point of maximum expiration.
- VC(Vital capacity): the volume of air breathed out after the deepest inhalation.
- VT / TV (Tidal volume) :the volume of air moved into or out of the lungs during quiet breathing (VT indicates a subdivision of the lung; when tidal volume is precisely measured, as in gas exchange calculation, the symbol TV or VT is used.)
- FRC(Functional residual capacity): the volume in the lungs at the end-expiratory position.
- RV/TLC% :Residual volume expressed as percent of TLC.
- VA :Alveolar gas volume.
- VL: Actual volume of the lung including the volume of the conducting airway.
- FVC(Forced vital capacity) : the determination of the vital capacity from a maximally forced expiratory effort.
- FEVt(Forced expiratory volume time ) a generic term indicating the volume of air exhaled under forced conditions in the first t seconds.
- FEV1: Volume that has been exhaled at the end of the first second of forced expiration.
- FEFx: Forced expiratory flow related to some portion of the FVC curve; modifiers refer to amount of FVC already exhaled.
- FEFmax :the maximum instantaneous flow achieved during a FVC maneuver.
- FIF (Forced inspiratory flow): Specific measurement of the forced inspiratory curve is denoted by nomenclature analogous to that for the forced expiratory curve. For example, maximum inspiratory flow is denoted FIFmax. Unless otherwise specified, volume qualifiers indicate the volume inspired from RV at the point of measurement.)
- PEF(Peak expiratory flow): The highest forced expiratory flow measured with a peak flow meter.
- MVV(Maximal voluntary ventilation): volume of air expired in a specified period during repetitive maximal effort.
INDICATIONS
Spirometry is indicated for the following reasons:
- To diagnose or manage asthma.
- To detect respiratory disease in patients presenting with symptoms of breathlessness, and to distinguish respiratory from cardiac disease as the cause.
- To measure bronchial responsiveness in patients suspected of having asthma.
- To diagnose and differentiate between obstructive lung disease and restrictive lung disease.
- To follow the natural history of disease in respiratory conditions.
- To assess of impairment from occupational asthma.
- To identify those at risk from pulmonary barotrauma while scuba diving.
- To conduct pre-operative risk assessment before anaesthesia or cardiothoracic surgery.
- To measure response to treatment of conditions which spirometry detects.
- To diagnose the vocal cord dysfunction.
CONTRAINDICATIONS
Forced expiratory maneuvers may aggravate some medical conditions. Spirometry should not be performed when the individual presents with:
- Hemoptysis of unknown origin
- Pneumothorax
- Unstable cardiovascular status (angina, recent myocardial infarction, etc.)
- Thoracic, abdominal, or cerebral aneurysms
- Cataracts or recent eye surgery
- Recent thoracic or abdominal surgery
- Nausea, vomiting, or acute illness
- Recent or current viral infection
- Undiagnosed hypertension
SPIROMETRY TESTING
The spirometry test is performed using a device called a spirometer, which comes in several different varieties. Most spirometers display the following graphs, called spirograms.
A volume-time curve, showing volume (litres) along the Y-axis and time (seconds) along the X-axis.
A flow-volume loop, which graphically depicts the rate of airflow on the Y-axis and the total volume inspired or expired on the X-axis.
PROCEDURE
The basic forced volume vital capacity (FVC) test varies slightly depending on the equipment used, either closed circuit or open circuit, but should follow the ATS/ERS Standardization of Spirometry.
Generally, the patient is asked to take the deepest breath they can, and then exhale into the sensor as hard as possible, for as long as possible, preferably at least 6 seconds. It is sometimes directly followed by a rapid inspiration, (inhalation) in particular when assessing possible upper airway obstruction. Sometimes, the test will be preceded by a period of quiet breathing in and out from the sensor (tidal volume), or the rapid breath in (forced inspiratory part) will come before the forced expiration.
During the test, soft nose clips may be used to prevent air escaping through the nose. Filter mouthpieces may be used to prevent the spread of microorganisms.
LIMITATIONS
The maneuver is highly dependent on patient cooperation and effort, and is normally repeated at least three times to ensure reproducibility. Since results are dependent on patient cooperation, FVC can only be underestimated, never overestimated.
Due to the patient cooperation required, spirometry can only be used on children old enough to comprehend and follow the instructions given (6 years old or more), and only on patients who are able to understand and follow instructions — thus, this test is not suitable for patients who are unconscious, heavily sedated, or have limitations that would interfere with vigorous respiratory efforts. Other types of lung function tests are available for infants and unconscious persons.
Another major limitation is the fact that many intermittent or mild asthmatics have normal spirometry between acute exacerbation, limiting spirometry’s usefulness as a diagnostic. It is more useful as a monitoring tool: a sudden decrease in FEV1 or other spirometric measure in the same patient can signal worsening control, even if the raw value is still normal. Patients are encouraged to record their personal best measures.
An abnormal ECG can mean many things. Sometimes an ECG abnormality is
a normal variation of a heart’s rhythm, which does not affect health.
Other times, an abnormal ECG can signal a medical emergency, such as a myocardial infarction /heart attack or a dangerous arrhythmia.
Abnormal results can signify several issues. These include:
- Defects or abnormalities in the heart’s shape and size:An abnormal ECG can signal that one or more aspects of the heart’s walls are larger than another meaning that the heart is working harder than normal to pump blood.
- Electrolyte imbalances:Electrolytes are electricity-conducting particles in the body that help keep the heart muscle beating in rhythm. If electrolytes are imbalanced, may have an abnormal ECG reading.
- Heart attack or ischemia: During a heart attack, blood flow in the heart is affected and heart tissue can begin to lose oxygen. This tissue will not conduct electricity as well, which can cause an abnormal ECG. Ischemia, or lack of blood flow, may also cause an abnormal ECG.
- Heart rhythm abnormalities: A heart typically beats in a steady rhythm. An EKG can reveal if the heart is beating out of rhythm or sequence.
- Medication side effects: Taking certain medications can impact a heart’s rate and rhythm. Sometimes, medications given to improve the heart’s rhythm can have the reverse effect and cause arrhythmias. Such as beta-blockers, sodium channel blockers, and calcium channel blockers.
ECG findings in First-degree heart block (AV block)
- First-degree heart block involves a fixed prolonged PR interval (>200 ms).
ECG findings in Second-degree heart block (type 1)
- Second-degree AV block (type 1)is also known as Mobitz type 1 AV block or Wenckebach phenomenon.
- Typical ECG findings in Mobitz type 1 AV block include progressive prolongation of the PR intervaluntil eventually the atrial impulse is not conducted and the QRS complex is dropped.
- AV nodal conduction resumeswith the next beat and the sequence of progressive PR interval prolongation and the eventual dropping of a QRS complex repeats
ECG findings in Second-degree heart block (type 2)
- Second-degree AV block (type 2)is also known as Mobitz type 2 AV block.
- Typical ECG findings in Mobitz type 2 AV block include a consistent PR interval durationwith intermittently dropped QRS complexes due to a failure of conduction.
- The intermittent dropping of the QRS complexes typically follows a repeating cycleof every 3rd (3:1 block) or 4th (4:1 block) P wave.
ECG findings in Third-degree heart block (complete heart block)
- Third-degree (complete) AV blockoccurs when there is no electrical communication between the atria and ventricles due to a complete failure of conduction.
- Typical ECG findings include the presence of P wavesand QRS complexes that have no association with each other, due to the atria and ventricles functioning independently.
- Cardiac function is maintained by a junctionalor ventricular pacemaker.
- Narrow-complex escape rhythms(QRS complexes of <0.12 seconds duration) originate above the bifurcation of the bundle of His.
- Broad-complex escape rhythms(QRS complexes >0.12 seconds duration) originate from below the bifurcation of the bundle of His.
ECG findings in Myocarditis :
The most common ECG abnormalities seen in myocarditis are:
- Sinus Tachycardia
- Non-Specific ST segment and T waves changes
- Prolonged QRS
- QT prolongation
- Diffuse T wave inversion
- Ventricular arrhythmias
- AV conduction defects
- With inflammation of the adjacent pericardium, ECG features of pericarditiscan also been seen (= myopericarditis)
ECG findings in Pericarditis :
- Widespread concave ST elevation and PR depression throughout most of the limb leads (I, II, III, aVL, aVF) and precordial leads (V2-6).
- Reciprocal ST depression and PR elevation in lead aVR (± V1).
- Sinus tachycardia is also common in acute pericarditis due to pain and/or pericardial effusion.
Changes in ST wave and its clinical importance
Tall sT waves
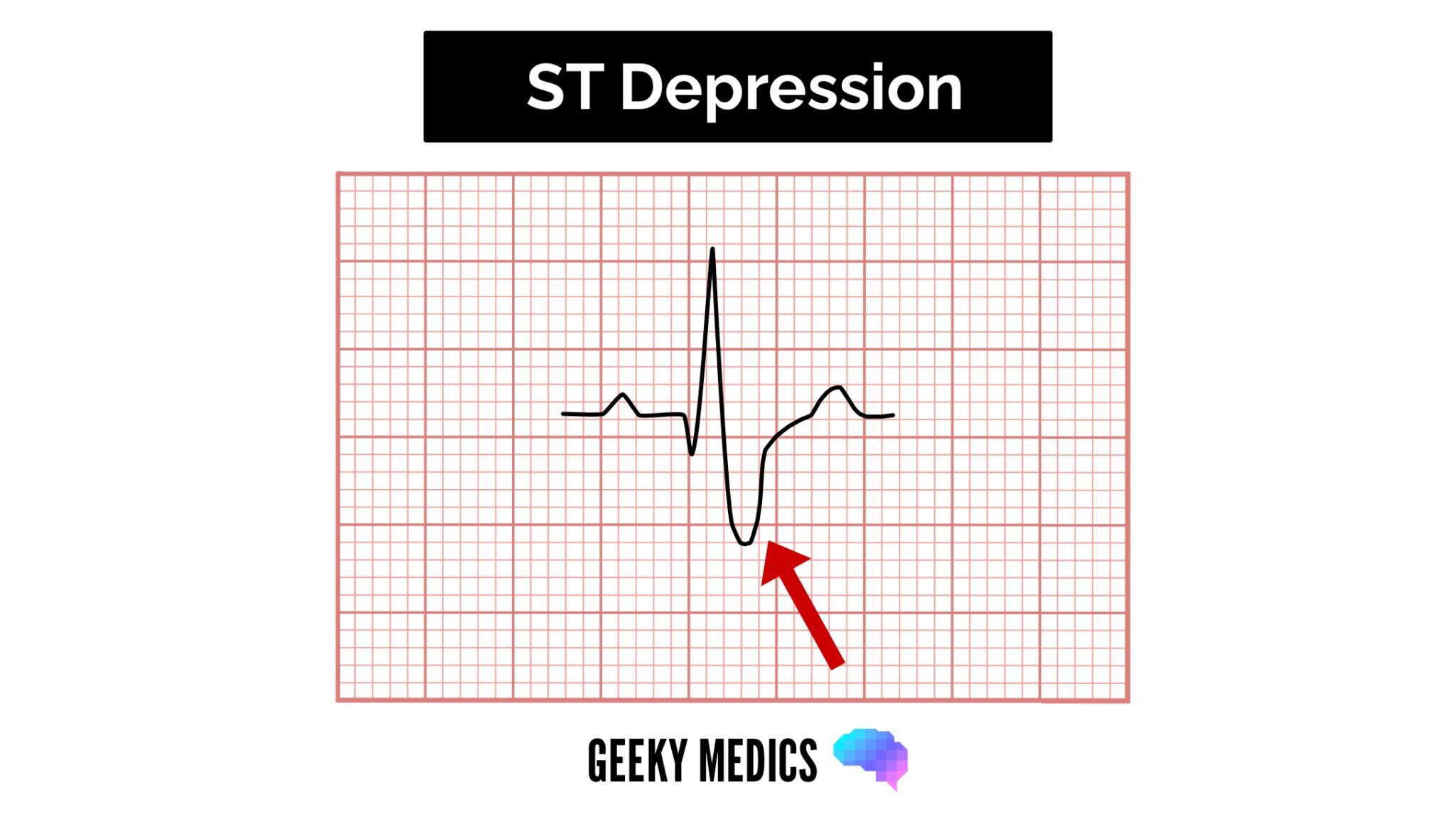
ST depression
{kind=link}
ST-elevation
- ST-elevationis significant when it is greater than 1 mm (1 small square) in 2 or more contiguous limb leads or >2mm in 2 or more chest leads.
- It is most commonly caused by acute full-thickness myocardial infarction.
- Anterior wall ST elevation MI
- ST segment elevation in the anterior leads at the J point and sometimes in septal or lateral leads depending on the extent of the myocardial infarction.
- Reciprocal ST segment depression in the inferior leads (II, III and aVF).
- Inferior wall st elevation MI
- ST segment elevation in the inferior leads (II, III, and aVF)
- Reciprocal ST segment depression in the lateral and/or high lateral leads (I, aVL, V5 and V6)
- Posterior wall st elevation MI
- ST segment depression in the septal and anterior precordial leads (V1 to V4). The ratio of the R wave to the S wave in leads V1 or V2 is > 1.
- ST elevation in the posterior leads of a posterior ECG (leads V7 to V9).
- ST elevation in the inferior leads (II, III, and aVF) may be seen if an inferior MI is also present.
Changes in T wave and its clinical importance
Tall T waves
T waves are considered tall if they are:
- > 5mmin the limb leads .
- > 10mmin the chest leads (the same criteria as ‘small’ QRS complexes)
Tall T waves can be associated with:
- Hyperkalaemia(“tall tented T waves”)
- HyperacuteSTEMI
Inverted T waves
- T waves are normally inverted in V1 and inversion in lead III is a normal variant.
- Inverted T waves in other leads are a nonspecific sign of a wide variety of conditions:
-Ischaemia
-Bundle branch blocks (V4-6 in LBBB and V1-V3 in RBBB)
-Pulmonary embolism
-Left ventricular hypertrophy (in the lateral leads)
-Hypertrophic cardiomyopathy (widespread)
-General illness
Biphasic T waves
Biphasic T waves have two peaks and can be indicative of ischaemia and hypokalaemia.
Flattened T waves
Flattened T waves are a non-specific sign, that may represent ischaemia or electrolyte imbalance.
Changes in u wave and its clinical importance
Tall T waves
- U waves are not a common
- The U wave is a > 0.5mm deflection after the T wavebest seen in V2 or V3.
These become larger the slower the bradycardia – classically U waves are seen in various electrolyte imbalances, hypothermia and secondary to antiarrhythmic therapy (such as digoxin, procainamide or amiodarone).
